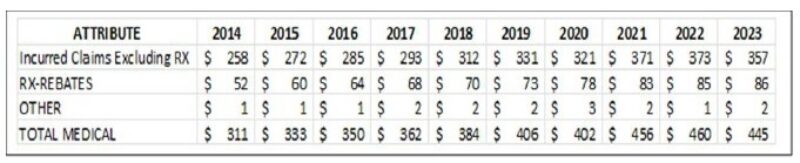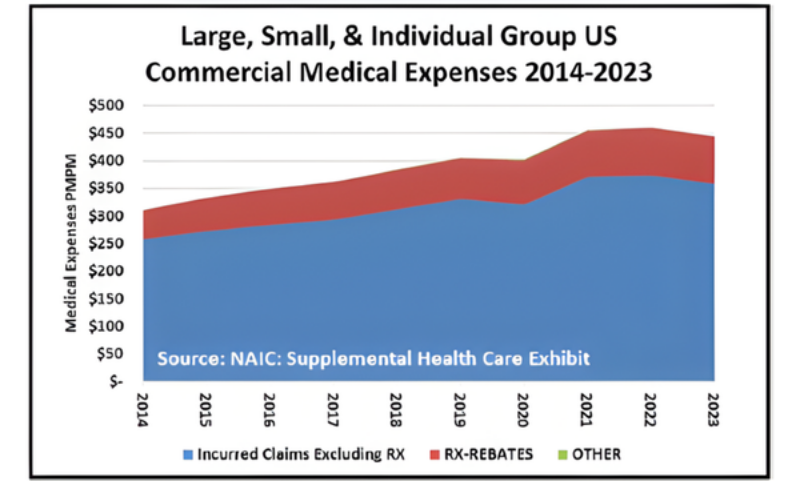
From 2014 to 2023, according to data from the NAIC, total commercial health-insurance medical costs rose from $311 to $445 per member per month (PMPM)—a 43 percent increase. Over that period, prescription drug spending (net of rebates) climbed from $52 to $86 PMPM, a 65 percent increase, while non-drug medical costs grew from $258 to $357 PMPM. Even so, drug costs accounted for only about one-quarter of the total dollar growth, while three-quarters came from hospital, system, and other medical services that receive far less public scrutiny.
Yet national debate continues to focus on drug prices because they are visible, quantifiable, and politically salient. This pattern embodies the “Drunkard’s Dilemma”—the tendency to search for solutions where the light is brightest rather than where the problem is largest. In health care, the streetlight shines on pharmaceutical spending, while most cost growth in dollars occurs in the shadows of hospital overhead, system transfers, and non-reimbursable expenditures.
A budgetary view of these data shows that drug spending, though significant, is not the primary driver of rising premiums. Employers, purchasers, and policymakers cannot achieve affordability by focusing solely on pharmacy costs. Progress will require payment reform, transparency in hospital and health system finances, and accountability for how new health-care dollars are used.
During this same period, the notion of health-care value moved to the forefront. Defining value—particularly hospital value—requires that a hospital’s impact on insurance premiums be visible and understood. Insurers can no longer react reflexively to annual percentage increases without examining their sources. In an era of scarce resources, we must know not only how much hospitals consumed, but what they used those resources for, and whether the spending advanced care quality or merely sustained inefficiency. True value depends on the efficient stewardship of every health-care dollar.